A Case of Compartment Syndrome
07 Nov 2018


It is important to seek early clinical assistance in making the diagnosis in problematic cases, and work towards an early surgical consensus as to how the condition should be managed.
Case study
A 30-year-old motorbike rider was brought to the ED following a collision with a pole. Injuries included extensive soft tissue thigh abrasions and a proximal fracture of his tibia on the same side with significant leg pain. The patient went to theatre for fixation of the tibial fracture and debridement of the thigh contusion that evening. An epidural was placed. The patient was monitored in ICU for other injuries.
The following day, a junior ICU doctor was asked to review the patient’s severe pain below his knee. A patchy epidural block was thought to be the cause. Following phone discussions with the Anaesthetist, further doses of the epidural (using a mix of local anaesthetic and opiate) were administered with good relief. That evening the pain returned. The epidural was turned off to allow proper assessment. The patient continued to experience uncharacteristically severe knee pain. Distal limb sensory loss was noted, initially attributed to the epidural, but eventually diagnosed as an acute compartment syndrome. The patient underwent fasciotomies.
The outcome was a permanent foot drop and sensory loss. Litigation was commenced two years later against the hospital (junior ICU doctor), Orthopaedic Surgeon, Intensive Care Specialist and Anaesthetist.
What is acute compartment syndrome (ACS)?
ACS typically results from the build-up of pressure within a muscle bundle encased in an inelastic fascial sheath. While there are physiological causes, e.g. exertional compartment syndrome, this discussion concentrates on ACS arising from injury or procedural interventions.
Causes are diverse, including trauma (both accidental, typically involving an underlying fracture, and iatrogenic, such as surgical intervention), spontaneous haemorrhage, venous or arterial circulatory obstruction, envenomation, local infection and external compression. While the lower limb is typically affected, other sites such as the abdomen and upper limb are also at risk.
Once compartment pressures exceed capillary filling pressures, a positive feedback mechanism develops, with ischaemia resulting in further increased compartment pressures, eventually impairing venous filling and then arterial perfusion. Without intervention, tissue necrosis of the compartment contents results. Occasionally external causes of increased pressure may contribute, such as splinting, plasters, dressings, circumferential burns or tourniquets.1
Long-term effects can include permanent loss of sensory and/or motor function, scarring and contractures, chronic wounds and infection (osteomyelitis), amputation and significant disfigurement. Surgical decompression (fasciotomy) to reduce the pressure in the compartments may release toxic by-products into the blood stream, impacting on other organs, causing renal failure, hyperkalaemia or even death.
Diagnosis
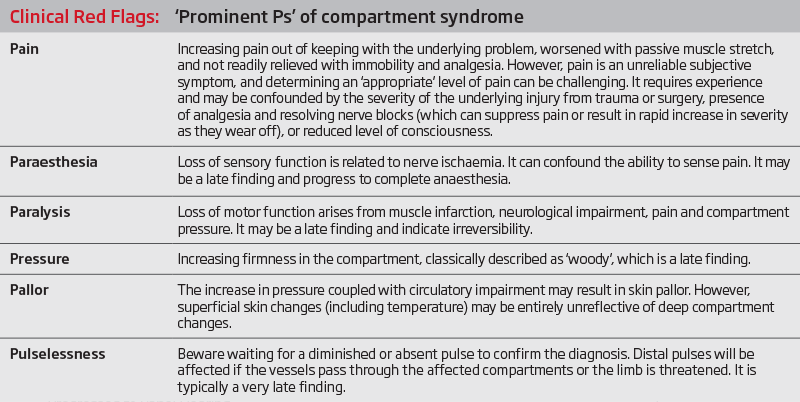
ACS should be treated as a surgical emergency. Diagnosis is primarily clinical and may be challenging, even for experts. Given the difficulties involved, early escalation and consultation should occur. Severe pain out of keeping with the underlying diagnosis, worsened with passive movement, is often the first sign. Many of the clinical ‘red flags’ have poor sensitivity, present late and have poor positive predictive value (often already present in many of the underlying injuries that create the risk). The appearance of ‘red flag’ symptoms may also herald that irreversible damage has already occurred. Intervention after 12 hours from symptom onset has been found to significantly reduce the chance of acceptable outcome to just 15%.2
Proper exposure and careful examination is critical including removal of anything which impedes review, e.g. casts, dressings or minimisation of regional nerve blockade.
If a clinical diagnosis cannot be made, pressure monitoring should be considered3 to exclude the diagnosis. However this may induce delays (and is considered to have low specificity4). Expertise in procedural setup may be lacking. A pressure gradient of <30mmHg between the diastolic blood pressure and compartment pressure is frequently cited as significant,5 but exact numbers vary.
Indirect supportive tests, e.g. creatinine kinase suggesting muscle breakdown, may be of assistance – but they typically indicate a late diagnosis and poor prognosis.
Certain scenarios should increase clinical suspicion. Tibial shaft fractures are well associated with ACS (ranging from 46-77% of such fractures and resulting in about 308-709% of ACS cases). Carefully consider scenarios involving concomitant anticoagulation or platelet inhibition.
There is recognition that once fulminant irreversible necrosis is inevitable, fasciotomy may increase the risk to the patient (by opening necrotic compartment, increasing the risk of deep infection, metabolic impacts) with little benefit. Our experience is that it is difficult to obtain peer support for failure to offer surgical decompression within the first 24 hours.
Medico-legal issues
These matters can be difficult to defend, particularly when they arise from failure to consider the diagnosis in the first place. A US 2004 review of 19 ACS claims found that fasciotomy performed within eight hours of symptom presentation uniformly resulted in successful defence.10 Data from a 2012 US review indicated 6% of all malpractice claims against Orthopaedic Surgeons were related to ACS.11 In the same review, the number of red flags present at the time of diagnosis correlates with increasing settlement value.
Exposure can occur for a wide range of treating clinicians, including ED doctors, hospital ward staff (nurses and doctors in training), Surgeons and Anaesthetists. Care should be taken to consider the appropriateness of regional anaesthesia in high risk cases.12 Early clinical consultation should be sought if the diagnosis is suspected.
The claims are often costly, involving permanent loss of function, cosmetic deformity, loss of limbs, and need for life-long prosthetics and rehabilitation. Given the underlying association with trauma, young patients are often involved.
Matters that are difficult to defend include:
- claimant aged between 16-35 years of age
- tibial fracture
- anterior compartment affected
- three clinical features apparent at an early stage
- diagnosis not entertained, or intervention delayed
- compartment pressure monitoring not undertaken before ruling out the diagnosis.
Conclusion
ACS remains a challenging diagnostic problem, but must be considered as a differential diagnosis in cases of atypically severe and persistent limb pain associated with tissue trauma. Seek early clinical assistance in making the diagnosis in problematic cases.
‘Time is muscle’ is the critical consideration, with delays in diagnosis of greater than 12 hours being associated with very poor outcomes. Work towards an early surgical consensus as to how the condition should be managed.
Dr Julian Walter
Medico-legal Adviser, MDA National

References
- McQueen MM, Gaston P, Court-Brown CM. Acute Compartment Syndrome. Who is at Risk? J Bone Joint Surg Br. 2000 Mar; 82(2):200-3. Available at: researchgate.net/publication/12561836_Acute_compartment_syndrome_Who_is_at_risk
- Hayakawa H, Aldington DJ, Moore RA. Acute Traumatic Compartment Syndrome: A Systematic Review of Results of Fasciotomy. Trauma. 2009 Jan 1. Available at: journals.sagepub.com/doi/abs/10.1177/1460408608099028
- Via AG, Oliva F, Spoliti M, Maffulli N. Acute Compartment Syndrome. Muscles Ligaments Tendons J. 2015 Mar 27;5(1):18-22. Available at: ncbi.nlm.nih.gov/pmc/articles/PMC4396671
- Hayakawa H, Aldington DJ, Moore RA. Acute Traumatic Compartment Syndrome: A Systematic Review of Results of Fasciotomy. Trauma. 1 Jan 2009. Available at: journals.sagepub.com/doi/abs/10.1177/1460408608099028
- Gadsden J, Warlick A. Regional Anaesthesia for the Trauma Patient: Improving Patient Outcomes. Local Reg Anesth. 2015 Aug 12;8:45-55. doi: 10.2147/LRA.S55322. eCollection 2015. Available at: dovepress.com/regional-anesthesia-for-the-trauma-patient-improving-patient-outcomes-peer-reviewed-article-LRA
- McQueen MM, Gaston P, Court-Brown CM. Acute Compartment Syndrome. Who is at Risk? J Bone Joint Surg Br. 2000 Mar; 82(2):200-3. Available at: researchgate.net/publication/12561836_Acute_compartment_syndrome_Who_is_at_risk
- Shadgan B, Pereira G, Menon M, Jafari S, Darlene RW, O'Brien PJ. Risk Factors for Acute Compartment Syndrome of the Leg Associated with Tibial Diaphyseal Fractures in Adults. J Orthop Traumatol. 2015 Sep; 16(3):185-92. Available at: ncbi.nlm.nih.gov/pubmed/25543232
- Gadsden J, Warlick A. Regional Anaesthesia for the Trauma Patient: Improving Patient Outcomes. Local Reg Anesth. 2015 Aug 12;8:45-55. doi: 10.2147/LRA.S55322. eCollection 2015. Available at: dovepress.com/regional-anesthesia-for-the-trauma-patient-improving-patient-outcomes-peer-reviewed-article-LRA
- Via AG, Oliva F, Spoliti M, Maffulli N. Acute Compartment Syndrome. Muscles Ligaments Tendons J. 2015 Jan-Mar; 5(1): 18–22. Published online 2015 Mar 27. PMCID: PMC4396671. Available at: ncbi.nlm.nih.gov/pmc/articles/PMC4396671
- Bhattacharyya, Vrahas. The Medical-Legal Aspects of Compartment Syndrome. J Bone Joint Surg. April 2004; 86:4; 864-868. Available at: journals.lww.com/jbjsjournal/Abstract/2004/04000/The_Medical_Legal_Aspects_of_Compartment_Syndrome.29.aspx
- Taylor RM, Sullivan MP, Mehta S. Acute Compartment Syndrome: Obtaining Diagnosis, Providing Treatment, and Minimizing Medicolegal Risk. Curr Rev Musculoskelet Med. 2012 Sep; 5(3): 206–213. Available at: rd.springer.com/article/10.1007%2Fs12178-012-9126-y
- Gadsden J, Warlick A. Regional Anaesthesia for the Trauma Patient: Improving Patient Outcomes. Local Reg Anesth. 2015 Aug 12;8:45-55. doi: 10.2147/LRA.S55322. eCollection 2015. Available at: dovepress.com/regional-anesthesia-for-the-trauma-patient-improving-patient-outcomes-peer-reviewed-article-LRA

Professional boundaries in healthcare - Part 1
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025

Understanding Professional Medical Indemnity Insurance
Do you understand the ins and outs of professional medical indemnity insurance?
11 Aug 2025

Professional boundaries in healthcare - Part 2
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025
Understanding Voluntary Assisted Dying laws
What are the laws and processes in place for VAD and what is my role?
22 Jul 2025