Improving the Quality and Safety of Bariatric Surgery
29 May 2018

This may be with the purpose of tracking a medical device, disease state or a particular procedure. When these variables are collected utilising pre-defined quality indices that have been agreed upon by experts as being clinically relevant and important, the benchmarked risk-adjusted data may be a valuable resource for providing feedback on outcomes to practitioners, patients, health services and device manufacturers.1
There are examples of feedback from clinical registries positively influencing patient care:
- The Australian National Joint Registry identified a poorly performing hip prosthesis that was ultimately withdrawn from the market.2
- Feedback from the Victorian State Prostate Cancer Registry has contributed to improved patient care and fewer positive surgical margins noted over a five-year reporting period.3
Bariatric surgery is a relatively young specialty and the procedures used are evolving rapidly. Unlike the introduction of new medications, new surgical procedures are usually introduced without high level of evidence supporting them, and with limited long-term data. Obesity is our most prevalent disease with 28% of Australian adults affected. This means there is high demand for the surgery, with demand at times outstripping the evidence base. This situation places patients at risk.
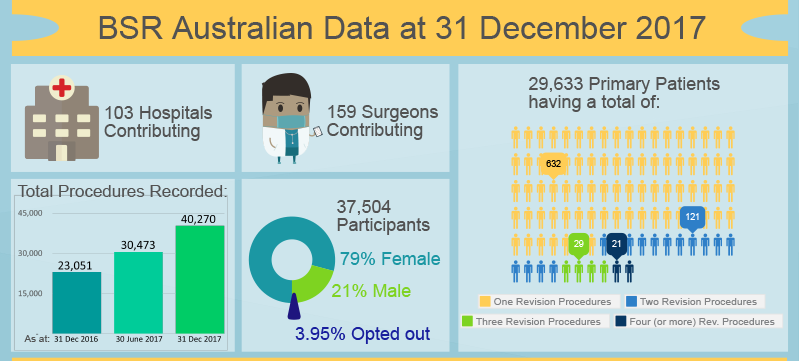
Recognising this risk, the Australia and New Zealand Bariatric Surgery Registry (BSR) was established by the Obesity Surgery Society of Australia and New Zealand (OSSANZ, now ANZMOSS) in partnership with Monash University, with the aim of monitoring the quality and safety of bariatric surgery in our countries, and using this data to improve outcomes. The pilot commenced in 2012. On the basis of this pilot, the Commonwealth Government funded a national rollout across Australia which is now almost complete. Rollout in New Zealand has commenced with the support of the device industry.
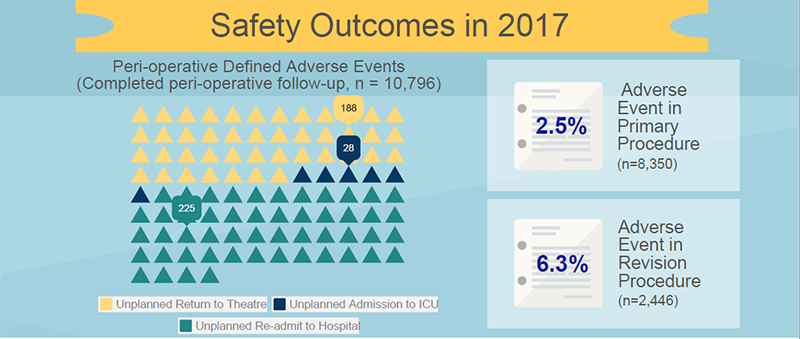
To minimise the potential for bias, it is important to make every effort to enrol all patients undergoing bariatric surgery in both countries, as well as to ensure every data field has near complete capture. For this reason, an opt-out process for patient consent has been utilised4 and only a few outcome measures are collected. We collect demographics, operative details, device details, BMI and diabetes status at baseline. At 90 days, clinical indicators are recorded. At annual follow-up, we record weight, diabetes status and need for reoperation. Deaths may be reported at any time. Outcomes are reported through a de-identified annual report as well as individual, benchmarked reports to all participating surgeons.
Images reproduced with permission from the Bariatric Surgery Registry as part of the School of Public Health and Preventive Medicine, Monash University
Working on the principle of early recognition, the registry aims to identify performance that is more than two standard deviations from the normal. These “outlying” surgeons, procedures, devices or hospitals are managed through a three-step process involving validation of data and then feedback to the involved party with the aim of identifying issues and improving performance. If performance continues to be poor after these steps are taken, the involved party will be reported to the relevant regulatory authority.
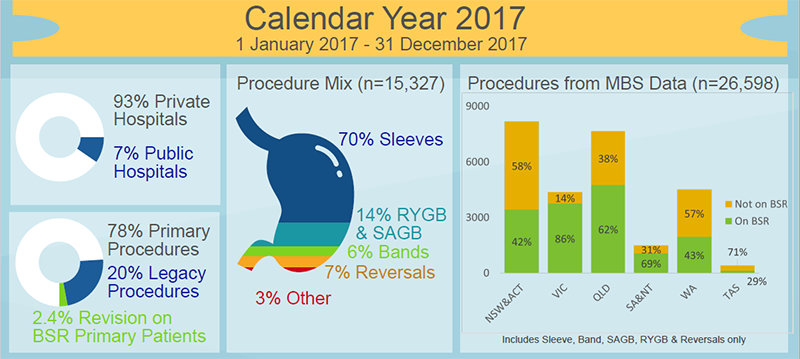
The BSR has now captured over 40,000 procedures. We anticipate that by the end of this calendar year, we will have completed our rollout across Australia and New Zealand. Our pilot cohort is reaching five years post-surgery. This data, collected purposefully and prospectively across the whole population, will give us an unprecedented opportunity to provide the community with information on the outcomes of these operations and the change in diabetes in this population.
Based on the experience of other registries, it is hoped that by feeding back the data to all interested parties we will see an improvement in the quality and safety of bariatric procedures undertaken in our community. We would encourage all Bariatric Surgeons to participate in this important initiative.
 Prof Wendy Brown (Guest writer)
Prof Wendy Brown (Guest writer)
Head, Monash University Department of Surgery
Director, Centre for Obesity Research and Education (CORE)
Clinical Lead, Bariatric Surgery Registry
 Prof Ian D Caterson (Guest writer)
Prof Ian D Caterson (Guest writer)
Director, Boden Institute, Charles Perkins Centre, University of Sydney
Director, Charles Perkins Centre Royal Prince Alfred Clinic
President, World Obesity Federation
References
- Brown WA, MacCormick AD, McNeil JJ, Caterson ID. Bariatric Surgery Registries: Can They Contribute to Improved Outcomes? Current Obesity Reports 2017;6:414-9.
- de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. The Journal of Bone and Joint Surgery American volume 2011;93:2287-93.
- Sampurno F, Earnest A, Kumari PB, et al. Quality of care achievements of the Prostate Cancer Outcomes Registry-Victoria. Med J Aust 2016;204:319.
- Tu JV, Willison DJ, Silver FL, et al. Impracticability of Informed Consent in the Registry of the Canadian Stroke Network. New England Journal of Medicine 2004;350:1414-21.

Professional boundaries in healthcare - Part 1
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025

Understanding Professional Medical Indemnity Insurance
Do you understand the ins and outs of professional medical indemnity insurance?
11 Aug 2025

Professional boundaries in healthcare - Part 2
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025
Understanding Voluntary Assisted Dying laws
What are the laws and processes in place for VAD and what is my role?
22 Jul 2025