You’re not Your Doctor - and I’m not Mine!
04 Nov 2014
A 26-year-old male surgical intern complaining of 5/10 peri-umbilical abdominal ache of semi-rapid onset post-bangers and mash for lunch presented to his GP seven days later.
The episode was preceded by three to four days of rhinorrhea, sore throat and a weekend ward call shift that included assisting in a laparoscopic appendectomy. The intern was severely lacking food, water, personal breaks and general sit-down time
Other associated features were feeling mildly feverish and nauseous but no vomiting, headache, loss of appetite or changes in bowel habit whilst the pain was exacerbated by lying supine but not relieved by the usual methods.
Intern’s self-diagnosis
Naturally, the provisional diagnosis was an easy one – mesenteric adenitis. After all, who would want to self-diagnose something so inconvenient as acute appendicitis, let alone in the middle of their surgical rotations during the first half of their internship?
If I confess that the eventual red flag symptoms of night-time awakening and migration of pain to the right iliac fossa did prompt me to face up to reality and seek a third-party medical opinion, perhaps you won’t deem me so incompetent that I couldn’t even diagnose my own appendicitis.
The importance of objectivity
Surely, as the ultimate possessor of information about one’s own symptomatology and past medical history, an individual armed with even a bit of medical knowledge care of Dr Google would be best placed to make the correct diagnosis? After all, we’re all taught “80% of diagnoses are made from taking a good history”. Well, as I learnt firsthand (and quite uncomfortably), even armed with a medical degree and some, albeit limited experience dealing with the presenting complaint of interest, without the objectivity of a thorough clinical examination and judicious investigations, one’s interpretation of their history for self-diagnosis is muddled by the diagnostician’s personal conflict of interest. We may be wanting to be well, or in other cases wanting to be unwell.
Take for example, some of the subjective “noise” experienced by the author in this instance.
It would be too ironic for me to have appendicitis during my surgical rotation let alone the inconvenience…
I don’t want to have appendicitis and definitely don’t want to need surgery because I like my old belly button…
Self-examination
Needless to say, self-examination can suffer the same fate of failing the objectivity test.
- Patient looked lousy in the mirror.
- Difficult to palpate/percuss one’s own abdomen without tensing – or was that guarding?
- Bowel sounds present – where’s the fridge?
I shall leave the ethical, legal and professional issues of ordering tests for oneself (or relatives) and self-prescribing for another time but by this stage in the author’s illness journey, the sensibleness of seeing his GP had triumphed. I acknowledged that my own pain and malaise was slowing my performance and if I continued, I would run the risk of reduced concentration impairing my ability to care for my patients with potentially harmful consequences for both parties. This was bearing in mind that peritonitis secondary to a ruptured viscus such as from appendicitis is a potentially fatal condition.
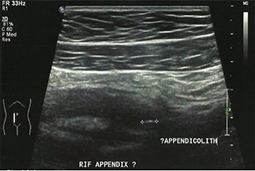
A proper, subjective history of the presenting complaint combined with knowledge of my past history and an objective clinical examination – Ouch! Yes, that was guarding and rebound tenderness – justified the ordering of a FBC, U&E, LFT and CRP as well as abdominal ultrasound. Sure enough, there was the mesenteric adenitis I had self-diagnosed… closely related to a 15mm thick appendix and appendicolith that needed to come out.
Returning to work
Eight days later, appendixless but sporting a shiny (bruised) new belly button, I was able to return to work having been cleared to perform CPR. This is the unofficial litmus test for returning to work as a resident medical officer post-abdominal surgery. However, I returned with heightened empathy for my patients, especially those with abdominal pain requiring surgery, as well as a critical reminder to seek professional, third-party medical opinion even (and perhaps, especially) as a doctor.
We make awful self-diagnosticians and even worse patients and may run the risk of harming our own health and wellbeing, as well our patients. Consider the analogy of fitting your own oxygen mask before tending to others and beware the temptation to neglect your own health by working yourself into the ground just to rival the ill health of your patients for the sake of building empathy. I would much rather read an illness narrative for this purpose than to experience it myself where it could be prevented. Please remember, doctors are only human, prone to sickness from time to time, no matter how high or fast you ascend the medical hierarchy.
So if pain persists, or any other constellation of signs and symptoms, please see your doctor, GP, surgeon or call 000.


Professional boundaries in healthcare - Part 1
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025

Understanding Professional Medical Indemnity Insurance
Do you understand the ins and outs of professional medical indemnity insurance?
11 Aug 2025

Professional boundaries in healthcare - Part 2
Boundaries with patients present in numerous ways every day and all health practitioners
11 Aug 2025
Understanding Voluntary Assisted Dying laws
What are the laws and processes in place for VAD and what is my role?
22 Jul 2025